Program Evaluation Proposal for Private Practice Merle Canfield, PhD
This is an outcome study proposal for an individual psychotherapy practice (or group practice). Six different packages or plans are offered to evaluate effectiveness for 100 clients. Each plan contains the study design, a set of proposed instruments, a schedule of data collection, an overview of statistical analyses, and sample results of analyses. The plans range from a post hoc satisfaction survey to a prospective study relating treatment to outcome as mediated by chronicity.
Six measures or scales are attached. The scales are selected to include outcome (pre- and post-measures of patient functioning), patient satisfaction, measure of treatment (the kind and amount of treatment received by the patient), previous history of the patient treatment (the purpose is to obtain an index of chronicity), and information about the interpersonal network of the patient. The measures used will depend on the study plan selected.
The proposed measures are:
History of Psychological/Psychiatric Problems
Outpatient Satisfaction Questionnaire
The Psychosocial Assessment Scale (Adult or Child)
The Psychotherapy Process Questionnaire
The Psychotherapy Session Questionnaire
The Social Network Questionnaire
These scales are optimal for cost and effectiveness. However, s these are global measures and will not capture the totality of either treatment or outcome. Consequently, either the domains or the scales may be revised. Other outcome measures that are popular are the BPRS and the SCL-90. Administration time and test cost should be considered when making substitutions. For example, one might consider using the MMPI for an outcome measure but the administration time would prohibit a telephone follow-up. Further, the cost of the test and scoring would be significant when one considers that the test may be administered to each patient a minimum of three times.
The Outcome Study Purpose
The objectives of the project are to:
Measure the effectiveness of treatment by assessing patient improvement.
Establish a relationship between treatment and outcome as moderated by patient status and environmental characteristics.
Develop models to predict optimal outcomes based on the influence and interaction of patient status and treatment elements.
The project enables the therapist to:
Use empirical models to develop effective treatment plans and to make treatment decisions. Maximize the probability of improved patient well-being in the most efficient manner.
demonstrate effectiveness to payers (optimal treatment may be longer for some patients).
Present results to the scientific community to contribute to the fund of knowledge and thus enhance managed care prestige.
Present results to the community served leading to informed choices, thereby, strengthening the managed care reputation.
Summary of Variables, Method of Data Collection, Instruments Used in Data Collection
The following is a summary of categories to be assessed and the methods and instruments to be used in data collection. Table 1 outlines the (a) general information obtained, (b) time of collection, and
(c) instruments used for data collection. Table 2 provides the specific variables to be measured.
Table 1. Data Collection Program.
![]()
Category Measured Time Instrument
Pre-admission Status | Admission | History of | Psychological |
Problems; | |||
Demographics | Psychosocial | ||
Prognostic Indicators | Assessment Scale | ||
Patient Social Network | (Adult; Children) | ||
Psychosocial Functioning | Social | Network |
Questionnaire
Treatment Variables At Treatment Termination Outpatient Satisfaction Questionnaire;
and Diagnosis Psychotherapy Session
Questionnaire; Psychotherapy Process Questionnaire;
Outcome--Patient Network, Six Months from Psychosocial Assessment
Admission Psychosocial Assessment
Scale (Adult; Children)
Social Network Questionnaire
![]()
Instruments
The Psychosocial Assessment Scale (PAS) is a 23 item inventory that utilizes a nine point (0 to 8) Likert-type scale. The patient rates each item according to the scale ranging from "none of the time" to "all of the time." Factor analysis of this measure yielded the following seven factors: Psychological Distress, Quality of Life, Relationships, Employment Functioning, Substance Abuse, Basic Living Skills, and Financial Stability.
The Psychotherapy Session Questionnaire (PSQ) is a 20 item scale that measures the degree and type of psychotherapy that was administered during a psychotherapy session. The PSQ was developed to relate treatment to outcome.
As does the PSQ, the Psychotherapy Process Questionnaire (PPQ) is used to relate psychotherapy process to patient outcome. The PPQ is a 22 item instrument that the therapist completes by rating the degree to which he or she engaged in such therapeutic interventions and approaches as goal setting, confrontation, interpretation, reinforcement, emotional expression, homework, and so forth.
The Social Network Questionnaire (SNQ) consists of 31 items that assess the patient's personal interactions and the types and quality of those interactions. The questionnaire measures a broad social network including mate, family, friends and co-workers. The Social Network Questionnaire may be completed by the patient or administered in a telephone interview (Canfield & Canfield, 1993).
Table 2 Specific Variables to Be Measured
---------------------------------------------------------------------------------------------------------------------
---------------------- PRE-INTAKE STATUS
Demographics
Gender Marital Status
Prognostic Indicators
Age at First Outpatient Treatment
Age at First Hospitalization
Patient Network
Relationship with Mate
State of Residence
Religion
Number of Therapists
Total Number of previous therapy hours
Relationship with Family
Date of Birth
Years of Education
Number of Previous Hospitalizations
Total Number Days of Prior Hospitalizations
Relationships with Friends
Relationships with Co-workers
Living Conditions
Psychosocial Functioning
Psychological Distress
Quality of Life Employment
Functioning
Substance Abuse
Basic Living Skills
---------------------------------------------------------------------------------------------------------------------
---------------------- TREATMENT COMPONENTS
Therapist Medication
Number of hours of Individual Therapy
Patient's Perception of Therapy
Therapist's Perception of Therapy
---------------------------------------------------------------------------------------------------------------------
---------------------- FOLLOW-UP STATUS
Patient Network
Relationship with Mate
Psychosocial Functioning Psychologica
l Distress
Quality of Life Diagnosis
Relationship s with Family
Employment Functioning
Substance Abuse
Relationship s with Friends
Basic Living Skills
Financial Stability
Relationship s with
Co-workers
Living Conditions
Data Collection Overview
Data are collected at the following intervals: Intake
Last session
Six months after last session Data Collected at Last session
The following data categories are collected at last session: Pre-last session Status
Demographics Prognostic Indicators Psychosocial Functioning
Selected variables from the measures of pre-last session status are repeated at the six month and one year follow-up intervals. Changes in pre-last session status are used to evaluate the treatment program. Pre-last session status information is acquired from the Psychosocial Assessment Scale (PAS).
Data Collected at Last session
At last session, information collected includes the following: Patient's Perception of Therapy
Therapist's Perception of Therapy
Last session data are collected by office staff or therapist by using the following instruments: Outpatient Satisfaction Questionnaire (OSQ), Psychotherapy Session Questionnaire (PSQ), and Psychotherapy Process Questionnaire (PPQ).
Data Collected at Follow-up
Five and one-half months after last session, patients are mailed the Psychosocial Assessment Scale (PAS) and Social Network Questionnaire (SNQ). Approximately 40 percent of the mailed follow-up forms are typically returned by the patients. Two weeks beyond the initial mailing, patients who have not responded are contacted by telephone and reminded to complete
and return the two forms. Four weeks beyond the initial mailing, the remaining patients who have not responded are contacted by telephone and forms are completed by the telephone interviewer. This interview takes approximately 20 minutes.
The follow-up data include such variables as: Relationships with Mate, Family, Friends and Co-workers Living Conditions
Psychological Distress Quality of Life Employment Functioning Substance Abuse
Basic Living Skills Treatment Status
Final Outcome Report
The Final Outcome Report is prepared after the 100th patient has completed the six month followup questionnaires. It is a comprehensive integration of the broad categories measured (See Table 1) and the specific variables measured (See Table 2) by the six instruments. This report provides follow-up information for the total sample of patients who have completed the six month follow-up. The Final Outcome Report includes information regarding:
The program's relationship to patient outcome, such as: Improved patient functioning
Improved social network Improved living conditions Improved quality of life
Improved employment functioning Decreased substance abuse Improved basic living skills
RES Proposal Page 7
The relationship between type of treatment and outcome
The relationships of patient chronicity and acuteness to treatment and outcome The relationships between diagnosis, treatment and outcome.
This report is designed to capture the complexity and interaction of patients, environments and treatments. Some patients need more treatment than others to make equal gains. Although this seems self- evident, it is not always taken into account by third party payers. This type of evaluation would give evidence by using the prognostic variables as mediators in the relationship between treatment and outcome. For example, two patients might enter the hospital with general feelings of worthlessness. The acute patient might gain a sense of worth with one week of treatment while the chronic patient might gain a sense of worth with one month of treatment. These differential effects of treatment are taken into account in this design. The prognostic variables will be used to moderate the effect of treatment on outcome to provide a more accurate picture of the relationship.
Further questions to be answered by the analysis include: What is the comparative impact of the directive approaches and cognitive approaches? What are the differential effects of these two approaches on different patients? The directive approach might benefit one type of patient and be detrimental to another type of patient. The approach of the design is to test these differential effects.
Sample Report Excerpts
The following samples illustrate samples of the various analyses to be performed. Any of the variables in the system may be related to any other variable in the system. The researcher may test many relationships as hypothesized in the literature (Canfield, et. al., 1988).
Sample 1
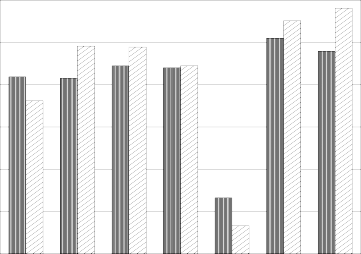
Figure 1 displays the means obtained from patients at last session and at six months on each of the seven PAS subtests. This example shows that on the average, patients improved in all areas measured by the Psychological Assessment Scale. It should be noted that for the Psychological Distress (DSTRS) and Substance Abuse (SUBAB) variables, the desired direction is a decrease. T-tests conducted on each pair of means demonstrate, with the exception of Employment Functioning, that the six month follow-up ratings are consistently (and statistically significantly) better than the ratings upon last session. These results suggest that the hospital treatment is beneficial to patients by reducing their psychological distress and substance abuse, and improving their quality of life, relationships, basic skills and financial stability.
RES Proposal Page 8
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
Figure 1. With the exception of employment, the last session score, in each case, is significantly different than the six month score.
RES Proposal Page 9
Sample 2
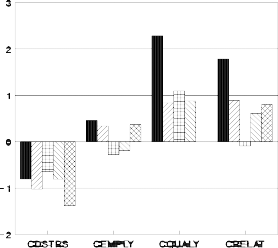
Figure 2 displays change scores between last session and the six month follow-up obtained from patients with different diagnoses. Affective, Anxiety, Borderline Personality Disorder, other Personality Disorders and Psychotic diagnoses are differentiated in their change scores on the Psychological Distress, Employment Functioning, Quality of Life and Relationship subtests. Psychological distress was decreased for all five diagnostic groups with patients diagnosed Psychotic showing the greatest reduction in perceived distress. Both Quality of Life and Relationships were generally improved, with patients suffering from affective disorders indicating the greatest changes. Interestingly, patients diagnosed Borderline showed no change in relationship functioning, and those diagnosed Psychotic showed no change in their Quality of Life from last session to follow-up.
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
Figure 2. Change scores of the Psychosocial Assessment Scale plotted by diagnosis.
RES Proposal Page 10
Sample 3
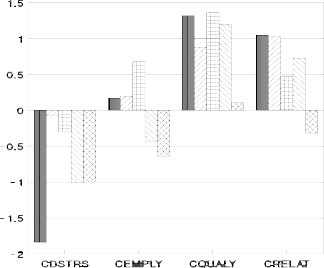
Figure 3 represents change scores by number of previous hospital last sessions. Treatment affects psychological distress, employment, quality of life and relationship factors differentially based on the chronicity of the patient. The number of previous hospitalizations was used as an indicator of chronicity experienced by patients. While all patients, regardless of previous number of last sessions, tended to report an improvement in their quality of life, first time last session patients showed the most significant reduction in psychological distress from last session to follow-up. Patients with four or more prior last sessions also showed a slight decrement in employment functioning following treatment, whereas, first, second and third time last session patients tended to improve in this area. On the Relationship subtest, all patients, except the most chronic (with five or more previous last sessions), improved.
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
Figure 3. Change scores on the Psychosocial Assessment Scale plotted by number of previous last sessions.
RES Proposal Page 11
Sample 4
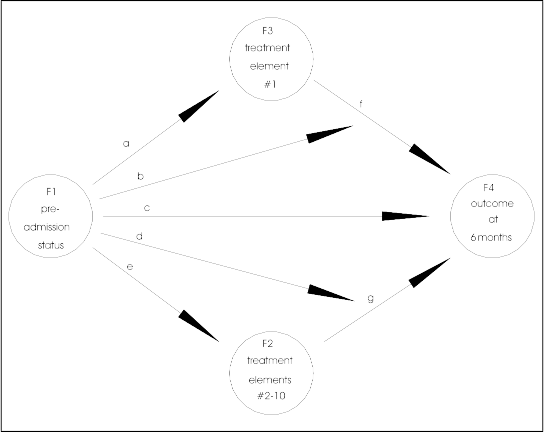
As we talked it seemed that it would be impossible to get treatment data (especially from charts), however, as Jerry and I looked at our instruments of assessing treatment implementation (the PPQ and PSQ) he thought that there might a possibility. At any rate I have included a track proposal for such a possibility. This design determines what elements of the treatment affect what elements of outcome for what type of patient. All of these elements--treatment, outcome and patient status--need to be measured. Historically, status and outcome have been extensively measured. Whereas, treatment has not been measured to this extent. The diagram in Figure 4 is used as a guide for this section.
Two concepts are important in assessing the effects of treatment on different types of patients. These concepts are: (a) mediation, and (b) interaction. Mediation is the effect of treatment or some other influence on the pre-last session status. If it were not for this mediation, it would be assumed that the status of the patient would not change so that at the six month follow-up the patient would be the same as at last session. For example, the score on Psychological Distress at last session (F1--pre-last session status) should be a predictor of Psychological Distress at six months follow-up (F4--outcome at six months). However, the six month score will be changed or "mediated" by treatment (F3--treatment element #1 and F2--treatment elements #2-10). The relative strength of these two mediating factors can be tested for their impact on outcome. Interaction occurs when patients differ in response to treatment. Some patients will be influenced by one treatment while other patients may not be influenced by the same treatment.
The analyses tests mediation and interaction. Consequently, the results will take the form of "block diagrams" representing these two concepts as illustrated in Figure 4. The circles represent factors of either status, treatment or outcome, and the arrows represent the direction of influence and interaction. When an arrow leads from one circle to another circle it represents the influence of one factor on another. When the arrow points to another arrow (e.g., "b" to "f"), it represents an interaction of the three factors connected by the arrows (e.g., F1, F3, and F4 in Figure 4). An example would be if Patient A (diagnosis phobic) were influenced by Treatment X, and Patient B (diagnosis schizophrenic) was not influenced by Treatment X.
Figure 4 shows a model to be tested. Each of the arrows (a through g) can be tested for the impact they represent. They can be tested individually or as part of the full model. For example, if all arrows but "c" were removed and "c" were found to be significant, one might conclude that the pre-last session status determines the outcome. That is, diagnosis, severity, degree of distress, etc. (F1--pre-last session status), predict outcome at six months (F4). However, if Treatment Element 1 (F3) is included (suppose that were individual therapy) then the significance of "c" is decreased or even reduced to 0. Further, Treatment Elements 2 though 10 (F2) could be added to assess the impact of Treatment Element 1. The arrows "b" and "d" represent interactions between patient status, treatment and outcome.
This example has represented one possible model to be tested. Many other models may be tested (see Canfield, et. al., 1988). The therapists in your group may want to generate a
RES Proposal Page 12
number of models based on their expectations and experience.
RES Proposal Page 13
Figure 4. A block diagram showing a possible model to be tested.
Proposed Plans
reports.
Table 3 outlines the time line for data collection and the preliminary, interim and final
Intake | Median Session | Last Session | Six Months | |
Plan I | OSQ | |||
Plan II | OSQ | |||
Plan III | PAS | PAS | ||
Plan IV | PAS HPP | PPQ PSQ PAS | PPQ PSQ PAS | |
Plan V | PAS | PPQ | PAS |
RES Proposal Page 14
HPP | PSQ | SNQ | ||
Plan IV | PAS HPP | PPQ PSQ | PAS SNQ |
OSQ Outpatient Satisfaction Questionnaire PAS Psychosoaical Assessment Scale
PPQ Psychotherapy Process Questionnaire PSQ Psychotherapy Session Questionnaire
HPP History of Psychological/Psychiatric Problems SNQ Social Network Questionnaire
Implementation
Implementation of the project, it will take somewhere between 2 to 4 months to begin data collection. The actual amount of preparation time will depend largely upon the therapist or the group. Time must be allotted to inform the therapists, solicit their participation, set up the system, train personnel, conduct a review process, and so forth.
Although the researcher has proposed specific instruments, the therapists may have suggestions for other instruments or other methods of gathering the same data. The researcher should work with the therapists in the use and/or development of different instruments. If the consultation becomes time consuming, then a consultation fee will be assessed. If this process becomes extensive, it could further delay the start of data collection.
Data Collection
Three of the questionnaires are completed by the therapists or their staff. Two of the questionnaires, the Psychosocial Assessment Scale (PAS) and the History of Psychological Problems (HPP), are administered at intake. The patients will usually complete the two questionnaires without assistance in about 15 minutes. In such cases, the staff time involves handing the questionnaires to the patient and retrieving them. On some occasions, the patient may be unable to complete the questionnaires (e.g., young children and non-readers), therefore, the person administering the questionnaires will need to interview the patient.
The two questionnaires that are administered at last session (PPQ and PSQ) are very similar to the last session questionnaires in terms of time and effort required. The administration of the questionnaire to the patient, again, must be timely in that it must be administered at or near the last visit. The questionnaire that the therapist (Psychotherapy Process Questionnaire) completes is not as critical in terms of time. Ideally, the therapist should complete PPQ at the time of last session. If patients return to therapy, they do not restart the process. They, instead, complete the 6 month administrations on their prior schedules.
The 6 month follow-up questionnaires are administered to the patient in the following
RES Proposal Page 15
manner. Five and one-half months from the time of last session (note that this is not five and one-half months from the last session of the patient), the patient is sent the PAS and SNQ with a request to complete the questionnaires and return them by mail. If the patient does not return the questionnaires, then a research assistant telephones and asks the patient if he or she has received the questionnaires and whether they have been completed. Frequently, the patient will complete the questionnaires at that time and return them. If the patient does not return the questionnaires after the first call, he or she is called again and interviewed by telephone with the research assistant completing the questionnaires. It should be noted that the letters sent to patients include a return card on which patients can indicate that they wish to be contacted by phone (or not at all). This process takes about one hour for each patient contacted.
There are six different plans as follows: Plan I.
In Plan I the Outpatient Satisfaction Questionnaire is administered to 100 patients at the last visit.
Plan II.
In Plan I the Outpatient Satisfaction Questionnaire is mailed to a sample of 500 former patients on a random basis. Means and standard deviations for each item of the questionnaire are provided and a short write up of the data
Plan III.
In Plan III the PAS is administered at intake and followed up six months later. The Outpatient Satisfaction Questionnaire is also administered at the six month followup. The questionnaires are mailed to 300 former patients, expecting a 30% return rate (it could be much lower). There are no telephone followups in this plan and consequently, approximately a 30% return rate might be expected and the study would be based on that 30%.
Plan IV.
In Plan IV the PAS and HPP are administered at intake, the PPQ, PSQ and PAS are administered at the "median session" and again at the last interview. 100 complete protocols are collected. There are no followup assessments. The report contains all elements of Samples 1, 2, 3, and 4 above. The analysis contains limitations because of the variability in the final assessment across patients. The assessment at the "median session" is an attempt to assess a "level playing field."
Plan V.
In Plan V the PAS and the HPP are administered at intake, the PPQ and the PSQ are administered at the last visit, and the PAS and SNQ are administered at followup. The questionnaires are mailed to 300 former patients, expecting a 30% return rate (it could be much
RES Proposal Page 16
lower). There are no telephone followups in this plan and consequently, approximately a 30% return rate might be expected and the study is based on that 30%. The report contains all elements of Samples 1, 2, 3, and 4 above.
Plan VI.
This plan is like Plan V except followup telephone calls will be made thus expecting a 50%
return rate (including the ones returned on the first mailing).
References
Canfield, M. L., Muller, J., Clarkin, J., Whitmarsh, J., Thorward, S. J., & Embretson, S. (1988). Issues in research design in psychiatric hospitals. The Psychiatric Hospital, 19, 11-26.
Canfield, M. L. & Canfield, J. E. (1993). A Collection of Psychological Scales. Bartlesville, OK: Research Evaluation & Statistics.
Canfield, M. L., Clarkin, J., Coyne, L., & Grob, M. (1987). Reliability of data taken from medical charts. The Psychiatric Hospital, 17, 173-179.
ATTACHMENTS
RES Proposal Page 17
Outpatient Satisfaction Questionnaire
Name:
Date:
Use the scale below to rate your satisfaction with therapy.
Completely Somewhat Satisfied Dissatisfied | Somewhat Completely Dissatisfied | Neutral Satisfied | ||||
8 | 7 | 6 | 5 | 4 | ||
3 | 2 | 1 | 0 | |||
0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | ... the progress that you have made? | |
0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | ... the interest your therapist showed in you? | |
0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | ... the problems that were solved in therapy? | |
0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | ... your level of comfort in therapy? | |
0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | ... the level of caring showed by your therapist? | |
0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | ... the suggestions made by your therapist? | |
0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | ... the plans made in therapy? | |
0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | ... the way that the therapist talked to you? | |
0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | ... the hope you were given by the therapist? | |
0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | ... the way the therapist understood you? | |
0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | ... the way the therapist keep your conversations private? | |
0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | I feel that therapy lasted longer than was necessary. | |
0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | Therapy was ended too soon to be useful. |
Circle the number that best represents the way you feel. How satisfied do you feel about...
0 1 2 3 4 5 6 7 8 I would recommend this therapy to my friends and family if they needed treatment.
0 1 2 3 4 5 6 7 8 Overall, I am satisfied with the treatment I received. Please use the back of this form for any comments you would like to add.
Psychosocial Assessment Scale
Name:
ID #
Date
Circle the number below that is the closest to how you have felt recently.
none all
IN THE PAST WEEK HOW OFTEN HAVE YOU ... of the several of the
time times time
...enjoyed your leisure hours (evenings, weekends, etc.)? 0 1 2 3 4 5 6 7 8
...felt fearful or afraid? 0 1 2 3 4 5 6 7 8
...felt sad or depressed? 0 1 2 3 4 5 6 7 8
...felt good about yourself or things you have done? 0 1 2 3 4 5 6 7 8 5. ...felt angry? 0 1 2 3 4 5 6 7 8
...felt mixed up or confused? 0 1 2 3 4 5 6 7 8
...felt like you've spent a worthwhile day? 0 1 2 3 4 5 6 7 8 8. ...felt tense? 0 1 2 3 4 5 6 7 8
9. ...felt useless? 0 1 2 3 4 5 6 7 8
very very
IN THE PAST WEEK ...
dissatisfied satisfied
...how satisfied have you been in general (with relationships, with finances, 0 1 2 3 4 5 6 7 8
and family?)
never often
...how often did you get together with people outside of your home? 0 1 2 3 4 5 6 7 8
all of
never the time
...did you handle the basic necessities such as paying bills, shopping and 0 1 2 3 4 5 6 7 8
and taking care of your room (home; apt.)?
none some much
...how much time did you spend with friends & family talking or doing things 0 1 2 3 4 5 6 7 8
together?
14. ...how much conflict was there with the person(s) you live with? | 0 1 2 3 | 4 | 5 | 6 | 7 | |
8 | ||||||
15. ...have you used alcohol? | 0 | 1 | 2 | 3 | 4 | 5 |
6 7 8 | ||||||
16. ...have you used drugs? | 0 | 1 | 2 | 3 | 4 | 5 |
6 7 8 | ||||||
-------------------- | ||||||
17. How much would friends or community members support you if you were sick | 0 | 1 | 2 | 3 | 4 | 5 |
6 7 8 | ||||||
or having problems? |
none some deal
employed time time
Are you employed (includes self-employed, housewife, student, employee)? 0 1 2 3 4 5 6 7 8
not part
not at all completely
Do you feel that you do a good job (whether self-employed, housewife, 0 1 2 3 4 5 6 7 8
student, employee)?
How much do you like your work (or studies)? 0 1 2 3 4 5 6 7 8
Do emotional problems interfere with your work (or studies)? 0 1 2 3 4 5 6 7 8
no enough
In the past month, was the amount of money you had, enough to pay the bills? 0 1 2 3 4 5 6 7 8
poor good
Do you feel that you are in good physical condition? 0 1 2 3 4 5 6 7 8
5-6-93
Name:
Patient:
Use the scale below to rate the way you usually respond in psychotherapy.
none of a little of some of a lot of all of
the time the time | the time | the time | the time | ||||
0 | 1 | 2 | 3 | 4 | 5 | 6 | |
7 | 8 |
IN PSYCHOTHERAPY SESSIONS WITH THE ABOVE PATIENT I:
0 1 2 3 4 5 6 7 8 helped the patient to identify specific goals of treatment.
0 1 2 3 4 5 6 7 8 worked toward specific goals.
0 1 2 3 4 5 6 7 8 intervened with family on behalf of the patient.
0 1 2 3 4 5 6 7 8 intervened with staff on behalf of the patient.
0 1 2 3 4 5 6 7 8 confronted the patient.
0 1 2 3 4 5 6 7 8 let the patient choose topics to talk about.
0 1 2 3 4 5 6 7 8 identified internal conflicts.
0 1 2 3 4 5 6 7 8 allowed tension to build between the patient and myself.
0 1 2 3 4 5 6 7 8 interpreted the patients thoughts and behavior.
0 1 2 3 4 5 6 7 8 allowed the patient to behave in a ways that I personally disagreed with.
0 1 2 3 4 5 6 7 8 gave "homework" to the patient.
0 1 2 3 4 5 6 7 8 had a plan of reinforcing the patient for positive behavior.
0 1 2 3 4 5 6 7 8 expressed disagreement with the patient.
0 1 2 3 4 5 6 7 8 talked about the "here and now".
0 1 2 3 4 5 6 7 8 asked questions about the patient's early development.
0 1 2 3 4 5 6 7 8 emphasized relationships.
0 1 2 3 4 5 6 7 8 talked.
0 1 2 3 4 5 6 7 8 felt close to the patient.
0 1 2 3 4 5 6 7 8 felt distant from the patient.
0 1 2 3 4 5 6 7 8 encouraged the patient to make his/her own choices.
0 1 2 3 4 5 6 7 8 set limits.
0 1 2 3 4 5 6 7 8 encouraged the patient to express repressed emotions.
Number of sessions completed:
Gender:
Date:_
Use the scale below to rate your MOST RECENT PSYCHOTHERAPY session.
Strongly Strongly
Disagree Disagree Neutral Agree Agree
0 1 2 3 4 5
6 7 8
Circle the number that best represents your attitude.
IN THE PSYCHOTHERAPY SESSION THE THERAPIST...
0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | was interested in me. |
0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | accepted our differences. |
0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | knew what I was talking about. |
0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | was comfortable. |
0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | was clear. |
0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | listened to me. |
0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | talked a lot. |
0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | made specific suggestions. |
0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | was on the same track with me. |
IN THE PSYCHOTHERAPY SESSION I...
0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | felt hopeful. |
0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | made a plan to deal with my problem(s). |
0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | felt better. |
0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | saw my problems as solvable. |
0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | moved toward my treatment goal(s). |
0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | recognized things that I didn't know about before. |
0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | felt involved. |
0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | saw things in new ways. |
0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | talked about my past. |
0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | talked about my relationships. |
0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | benefitted from therapy. |
History of Psychological Problems
Name: Address:
Date:
City:
State:
Zip:
Telephone: ( )
Therapist:
Date of Birth:
Gender:
Education:
Marital Status: Ethnicity: Religion:
Never Married (1) African-American (1) Catholic
Married (2) Asian-American (2) Jewish
Separated (3) European-American (3) None
Divorced (4) Hispanic (4) Protestant
Widowed (5) Native American (5) Other
Other
What is the problem or problems that brought you to treatment?
![]()
![]()
If you have never received psychotherapy or counselling then go to the next box.
At what age did you first receive psychotherapy or counselling?
How many different therapists have you received psychotherapy or counselling from?
Approximately how many hours of psychotherapy and/or counselling have you received altogether?
If you have never been admitted to an inpatient psychiatric hospital, substance abuse treatment, or other psychiatric treatment facility then skip this box.
At what age were you first admitted to an inpatient treatment facility?
How many times have you been admitted to an inpatient treatment facility?
Approximately how many total days have you received treatment in an inpatient treatment
facility?
Social Network Questionnaire
Name:
Age:
Gender:
For items numbered 1 through 24 consider the following people: spouse or mate, family, friends, people at work/school, or acquaintances. Leave the item blank if it does not apply to you. For example, if you are not married or living with someone, items 1 through 6 would be left blank. Think about each of those persons listed and the kind of activity you had with them. You should have an entry for each item according to the following:
8 = daily
7 = five or six times per week 6 = two to four time per week
5 = about once a week
4 = two or three times per month 3 = about once a month
2 = two to eleven times per year 1 = about once a year
0 = never
talk with | conflict with | close to | support from | productive activity | leisure activity | |
spouse or mate | 1. | 2. | 3. | 4. | 5. | 6. |
family | 7. | 8. | 9. | 10. | 11. | 12. |
friends/acquaintances* | 13. | 14. | 15. | 16. | 17. | 18. |
people at work/school | 19. | 20. | 21. | 22. | 23. | 24. |
feel
get
share in
share in
* NOTE: If some people are both co-workers (or classmates) and friends, then rate the time
spent with them outside of work (school) as friends and the time at work (school) as co-workers (or classmates).
My living condition is: (check one)
( ) Live with family
( ) Live alone
( ) Live with relative(s)
( ) Live in psychiatric institution
( ) Live in halfway house
( ) Live with someone other than relative
( ) Live in foster home